What Causes Scoliosis? Looking Beyond the Curve
One of the most frustrating aspects of scoliosis is when people discuss scoliosis and say its cause is unknown.
The majority of scoliosis diagnoses fall under the category of idiopathic scoliosis, which means “of unknown origin.” I am not a fan of this concept.
Several contributing factors may work alone or in combination to produce the complex, asymmetrical curvature of scoliosis. From genetics and growth patterns to muscle imbalances and nervous system dysfunction, the picture extends far beyond the spine itself.
The Many Faces of Scoliosis
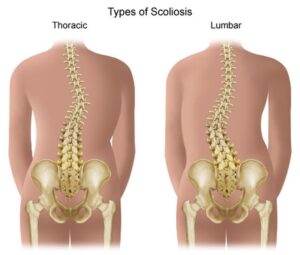
Let’s start by briefly reviewing scoliosis types:
- Idiopathic scoliosis (most common, particularly in adolescents). Idiopathic means that there is no known origin. What drives me crazy about this is that there is a reason for everything that happens in the body.
- That said, idiopathic scoliosis progresses relative to the rate of growth in children. As the body grows and develops and goes through growth spurts during puberty, curves progress fastest.
- Congenital scoliosis— curvature of the spine is present at birth, caused by abnormal development of the vertebrae during fetal development. Unlike other forms of scoliosis that develop later, this condition arises from issues like improperly formed or fused vertebrae.
- Neuromuscular scoliosis— the spine curves sideways due to underlying neurological or muscular disorders such as cerebral palsy, spina bifida, muscular dystrophy, or spinal cord injuries.
- Degenerative scoliosis— Degenerative scoliosis is a curvature of the spine that develops in adults due to wear and tear on the spine. Issues like stenosis, spondylosis, and degenerative disc disease can lead to changes in the spine and its alignment.
Each type may have different underlying causes, but several common contributors are worth highlighting—especially in idiopathic and adult-onset scoliosis.
Hypermobility and Connective Tissue

One often overlooked factor is hypermobility, a condition where joints move beyond the normal range of motion due to loose or stretchy connective tissue. People with hypermobility may appear “flexible” but lack the muscular control to stabilize their joints.
In a hypermobile spine, vertebrae may shift more easily out of alignment. If muscle support is insufficient or uneven, the spine may begin to curve. Over time, this asymmetry can become fixed. Conditions like Ehlers-Danlos Syndrome, a connective tissue disorder on the higher end of hypermobility issues, are frequently associated with scoliosis.
My own story is one of mild hypermobility, which ultimately cost me three knee surgeries before I figured out the source of my pain. As it turns out, many of the clients I now work with are also dealing with some combination of hypersensitivity and hypermobility.
Muscle Imbalances and Asymmetry
Muscles don’t just move the body—they also stabilize it. When certain muscles are chronically tight or overactive on one side, and weak or underactive on the other, the spine may begin to tilt or rotate.
The psoas, my favorite muscle, which is one of only three muscles connecting the legs to the spine, is especially relevant in scoliosis.
If one side of the psoas is tighter or more dominant, it can create torque through the pelvis and spine, drawing the lower spine into rotation and imbalance. Left unaddressed, this asymmetry can reinforce or even drive a scoliotic pattern.
Nervous System Involvement
The nervous system is everything when it comes to posture, movement coordination, and muscle tone.
Proprioception is the body’s internal sense of where it is in space. The vestibular system, by contrast, governs balance and spatial orientation. Difficulties with one or both of these functions can interfere with the body’s ability to adapt to growth and movement.
Over time, these challenges may contribute to the development of scoliosis, particularly by limiting the body’s capacity to make the subtle postural adjustments needed as we grow.
Nerve tension, also known as neural tension, is when nerves experience restricted mobility or become irritated due to various factors.
- Tumors or cysts can bind the spinal cord and cause a tension on the nerves, leading to scoliosis.
- Intraspinal anomalies: The spinal cord or nerves develop embryologically in a way such that one side or one part of the cord is pulled tight at birth. Even though the problem happens at birth, it might not manifest until growth kicks during puberty.
- Tethered Cord Syndrome: A condition from birth that causes the entire spinal cord to be pulled noticeably lower towards the sacrum, placing tension on the spinal cord.
- Uncoupled Neuro-Osseous Development: The spinal cord (neuro) is not growing as fast or as long as the bones of the spine (osseous).
The tension created by a tightened spinal cord can cause the spinal column to adapt by curving in relation to the tightened cord.
Growth and Genetics
In adolescents, scoliosis often appears during growth spurts—when bones grow faster than muscles and ligaments can adapt. This mismatch may allow curves to develop or worsen.
There is also a genetic component. If a parent or sibling has scoliosis, you are more likely to develop it. While no single gene has been identified as “the scoliosis gene,” multiple genes may contribute to its development and progression.
What causes scoliosis isn’t always one thing—it’s often a mosaic of biomechanical, genetic, neurological, and sometimes emotional factors.
In my next post, I’ll dive deeper into diagnosis and treatment—looking at when bracing makes sense, who might need surgery, and how to approach scoliosis from a movement-based perspective.