What Is Scoliosis? Understanding the Basics
I am debuting a new workshop in September on scoliosis: Understanding Scoliosis: Looking Beyond The Curve
My work is focused on walking, posture, and exercising correctly. While I am not a scoliosis expert, this series of blog posts aims to provide an overview of scoliosis, offering a deep understanding of its origins, effects, and options for rehabilitation.
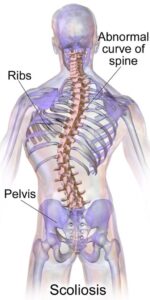
Scoliosis is a curvature of the spine, but that simple definition doesn’t quite capture the complexity of the condition. While the spine naturally has four curves—two curves that go in (lordosis) and two curves that go out (kyphosis) —scoliosis introduces abnormal curves in the coronal plane, which often also twist and rotate the spine in three dimensions.
Scoliosis can range from mild and barely noticeable to severe and physically disabling. Understanding its types, anatomy, and diagnostic tools is the first step toward a more informed and personalized approach to managing it.
The Anatomy of the Spine
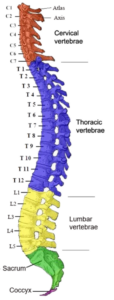
The human spine consists of 33 vertebrae stacked vertically and divided into five regions: cervical (neck), thoracic (mid-back), lumbar (low back), sacral, and coccygeal.
Between the vertebrae that are above the sacrum, there are cushiony intervertebral discs that provide shock absorption and flexibility.
Each vertebra also has a pair of facet joints that guide and limit movement, maintaining the spine’s alignment and stability.
When scoliosis develops, it alters how these structures bear weight and move, often leading to muscle imbalances, joint compression, and compensatory patterns throughout the body.
Types of Scoliosis and When They Occur
There are several distinct types of scoliosis, each with different causes and onset periods:
- Idiopathic Scoliosis: This is probably the most common and most frustrating form of scoliosis, especially in adolescents. “Idiopathic” simply means they don’t know why it occurs, though genetics and growth patterns are likely involved.
- Congenital Scoliosis: Caused by abnormal spinal development in the womb. This type is often present at birth and may worsen as the child grows.
- Neuromuscular Scoliosis: Linked to conditions like cerebral palsy, muscular dystrophy, or spinal cord injury, where muscles can’t support the spine properly.
- Degenerative Scoliosis: Also called adult-onset scoliosis, this occurs due to age-related spinal wear and tear. As discs and joints deteriorate, curves may develop later in life.
An important thing to understand is scoliosis is not a one-size-fits-all condition, and each type requires a unique management plan.
Measuring Scoliosis: The Cobb Angle
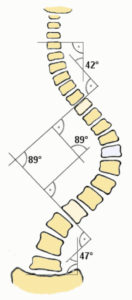
One of the most important tools for diagnosing and tracking scoliosis is the Cobb angle, a measurement taken from spinal X-rays. It quantifies the degree of spinal curvature by measuring the angle between the most tilted vertebrae above and below the curve. A Cobb angle of:
- 10° or more is considered scoliosis
- 20° to 40° may warrant observation or bracing
- 40° or more often triggers discussion about surgical intervention
The Cobb angle provides a standard for assessing severity, but it doesn’t capture everything. Two people with the same angle may experience scoliosis very differently.
The Adams Forward Bend Test
A common screening tool, especially in schools, is the Adams Forward Bend Test. The person bends forward from the waist, and the examiner looks for asymmetries in the ribcage or back—like a “rib hump.”
In future posts in this series, I’ll explore why no two curves are alike, what causes scoliosis to progress, and why generic exercises may not be enough. We’ll also dive into how the psoas, nervous system, and even hypermobility can play a role in shaping and supporting a spine with scoliosis.
For now, know this: scoliosis is far more than a curve. It’s a complex, multifactorial condition that deserves a thoughtful, individualized approach.